Medical Evacuations for Inuit Pregnant People: Reclaiming Inuit Birthing Practices
- Nov 16, 2023
- 5 min read
Updated: Dec 3, 2023

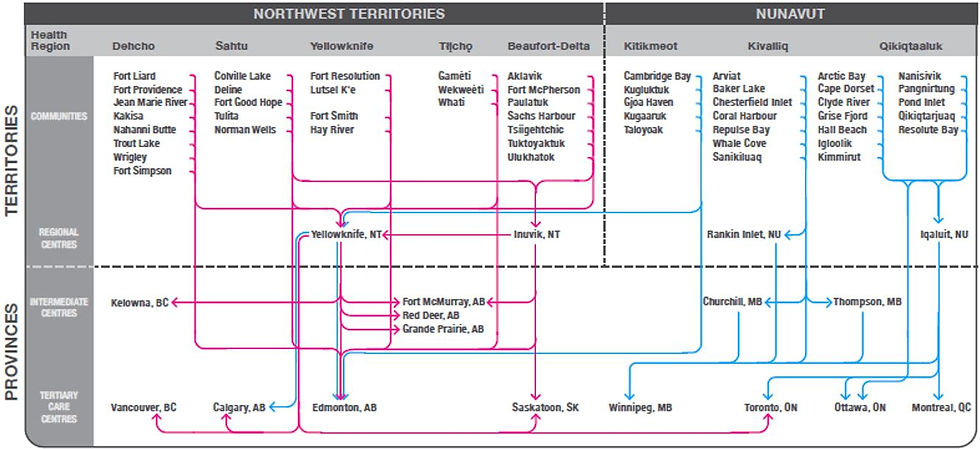
The Kivalliq region of Nunavut is the administrative area of southern Nunavut. It consists of the southern mainland border, the majority coastline of Hudon’s Bay, Southhampton Island, and Coats Island. It is ceilinged by the Northern Passage, which acts as a geographical end point to the Kivalliq region. There are 7 communities within Kivalliq: Arviat, Baker Lake, Chesterfield Inlet, Coral Harbour, Naujaat, Rankin Inlet, and Whale Cove. It is home to over 11’000 people who honour the lands and traditional ways of life with hunting, fishing, and living. Due to its remote location, large surface area and small population size, access to obstetrical services is limited and many pregnant Inuit people are medically evacuated to Winnipeg, Edmonton, Churchill, or Iqaluit for perinatal and birthing services between 36- and 38 weeks gestation (Clark et al., 2022). This mandate was proposed in the spirit of improving
perinatal and postnatal health, however little regard was given to the emotional, economic, and social changes, or to individual preferences
(Lavoie et al., 2022). As a result, medical evacuations have altered the traditional ways of life and deeply affected patient experience and connection to the land and community in unforeseen ways.
This medical evacuation is promoted by governmental authorities to improve access to perinatal and birthing services; however, it mimics eerily the forced removal of children from homes during the times of residential schools and ongoing practices by welfare services (Dreaddy, K. 2019). This colonial medicalization of Inuit and Indigenous health is linked with psychological, physical, and social deterioration, as pregnant people are evacuated without their birthing partners or support systems and forced into Western medical systems without traditional knowledge or practices (Lee et al., 2020; Lavoie et al., 2022). With the extended relocation, there is increased pressure on local resources, reinforcing issues of food scarcity, home security, and increased Territorial health expenses (Lee et al., 2022; Dreaddy, K. 2019). This practice has been linked to serious psychological impacts on pregnant people, including higher rates of depression, anxiety, sense of isolation, and feeling removed from their natal lands and belief systems (Dreaddy, K. 2019). This can create a negative experience around birthing, which can often perpetuate inter-generational trauma.
Traditionally, delivery was a natural connection to the world, supported by entire community systems and often attended by many attendants, including Elders, ikajurti, and husbands. Many people were trained to provide natal care due to the remoteness and high likelihood of isolated or independent birthing. In the 1970s, Western nurses were routinely sent to Nunavut to provide support to pregnant people, and it became illegal to offer midwifery or ikajurti services in a region with a physician (Lee et al., 2020). This made it difficult to pass on these skills, and a separation of generations, Inuit traditional knowledge, and spiritual practice was intentionally stifled. The shift towards medical prenatal evacuations undermined the ikajurti, the traditional midwifery practice (Lee et al., 2020).
In 1876, the Indian Act was passed which gave unprecedented control to governments and infiltrated every imaginable sector of Indigenous life (Dreaddy, K., 2019). It promoted the Westernization of medical services, belittling or negating traditional knowledge and practices (Matheson et al., 2022). The practice led to an unprecedented amount of governmental surveillance on individuals and has been tied to a disproportionate number of Inuit children being removed from their homes at or around the time of their birth (Dreaddy, K., 2019). Forced medical evacuation speaks to the historical mistreatment of Indigenous and Inuit People in Canada, as it instilled mistrust and fear in government systems and perpetuated intergenerational trauma.

Up to 91% of Kivalliq pregnant people are removed from their communities for birthing services, costing the Nunavut government $3.7M in transportation and out-of-territory medical expenses (Dreaddy, K., 2109). Despite community advocacy to improve perinatal access and local delivery services, the current evacuation processes are unlikely to change due to staffing shortages, high turnover rates due to working conditions, isolation, extended scope of practice demands, and high cost of living (Lee et al., 2020; Lawford & Giles, 2016). This leads to an
over-reliance on short-term locums and an inter- generational disconnect from traditional birthing practices and land birth connection,
an integral part of the Inuit and Indigenous belief system (Lavoie et al., 2022).
There is a newfound shift of support for Inuit remote communities, particularly in the Kivalliq region, as Inuit pregnant people and traditional ikajurti knowledge keepers advocate for more inclusion of traditional birthing practices to be incorporated in Inuit births (Dreaddy, K., 2019). There are many institutions which promote Inuit midwife licensing, including Dalhousie University which has an Iqaluit-based program specifically designed to blend evidence-based Western medical practices with generations-old Inuit knowledge. Encouraging Inuit midwives helps to foster services in remote communities, addressing the unique logistical needs of these communities and helping to offset employment instability and short-staffing limitations (Lee et al., 2022). It also provides birthing instructions in Inuktitut which is integral to the vast majority of patients for whom this is their natal language (Lee et al., 2022). It is important to note that post-natal outcomes for low-risk pregnancies are very promising when coupled with experienced midwives (Moran& McCue, 2023). Nunavut hosts significantly lower Cesarian section rates and has a similar poor outcome rate as the rest of Canada, reinforcing that force evacuations for low-risk pregnancies do not provide the superior medical care as initially promoted (Lee et al., 2022). However, limited research has been conducted into the natal outcomes of evacuated Indigenous People versus non-Indigenous People.

Forced evacuation of pregnant Inuit people has been a gold standard in the Kivalliq region of Nunavut since the 1980s, a tribute to Western medicalization and colonial views. It has been linked with psychological distress as pregnant people are removed from their hometown, birth partners, supporting community and birthing traditions. As a result, there are increased rates of parental anxiety and depression, as well as the sensation of cultural and physical isolation at an already vulnerable time. These practices add economic pressure on Territorial healthcare resources due to medical air evacuation and out-of-territory accommodation and medical expenses. Despite this, natal outcomes are not significantly better when compared with Inuit midwife-assisted births, supporting the need for additional research into this potentially archaic and harmful practice, as well as the need to support more Inuit midwives in remote communities.
References
Clark, W., Lavoie, J.G., McDonnell et al., (2022). Trends in Inuit Health Services Utilisation in Manitoba: Findings from the Qanuinngitsiarutiksait Study. International Journal of Circumpolar Health, 81(1). doi: 10.1080/22423982.2022.2073069
Dreaddy, K. (2019). Indigenous Obstetric Evacuation: Harmful but Risky to Resist. Impact Ethics. https://impactethics.ca/2019/12/19/indigenous-obstetric-evacuation-harmful-but-risky-to-resist/
Grant, K. (2021). In Nunavut, a Push to blend Traditional Inuit Birthing Practices with Modern Doula Care. The Globe and Mail. Retrieved https://www.theglobeandmail.com/canada/article-keeping-the-spirit-of-traditional-inuit-birthing-practices-alive/
Lavoie, J.G., Clark, W., McDonnell, L. et al (2022). Kivalliq Inuit Women Travelling to Manitoba for Birthing: Findings from the Qanuinngitsiarutiksait Study. BCM Pregnancy and Childbirth, 22:870. https://doi.org/10.1186/s12884-022-05214-9
Lawford, K.M & Giles, A.R. (2016). Kivalliq Inuit Centre Boarding Home and the Provision of Prenatal Education. International Journal of Circumpolar Health, 9(75). doi: 10.3402/ijch.v75.32213
Lee, E., Gudmundson, B., & Lavoie, J.G. (2022). Returning Childbirth to Inuit Communities in the Canadian Arctic. International Journal of Circumpolar Health, 81(1). doi: 10.1080/22423982.2022.2071410
Moran, P. & McCue, D. (2023). Hands of a Midwife. CBC Radio One. Hands of a midwife (cbc.ca)




Comments